
 ersonal interests in the medical world make me do a lot of research in this field, especially in the history of medicine and how it has evolved over the years. If you would have told me that back in the 19th century when slavery was still common, society believed that Black people were more resilient to pain than white people I would have understood the origin of this misconception. However, what truly surprised me is to find out that not only is this myth still believed to this day, but also that international medical schools are still teaching this lie!
ersonal interests in the medical world make me do a lot of research in this field, especially in the history of medicine and how it has evolved over the years. If you would have told me that back in the 19th century when slavery was still common, society believed that Black people were more resilient to pain than white people I would have understood the origin of this misconception. However, what truly surprised me is to find out that not only is this myth still believed to this day, but also that international medical schools are still teaching this lie!
Before portraying the way society still believes this myth I want to show you where this myth started from or better said who gave birth to this myth. For this we need to go back to the beginning of the 19th century, to be more specific 1820s.
The birth of this myth
The man who is credited for the birth of this myth is Dr. Thomas Hamilton who had an ongoing obsession with proving the “differences” between white people and Black people on a psychological level as much as a physical level. To do this Hamilton performed excruciatingly painful medical experiments that in his mind would showcase the results of Black people feeling less pain than white people because his theory described that Black people have thicker skin and less sensitive nerves.
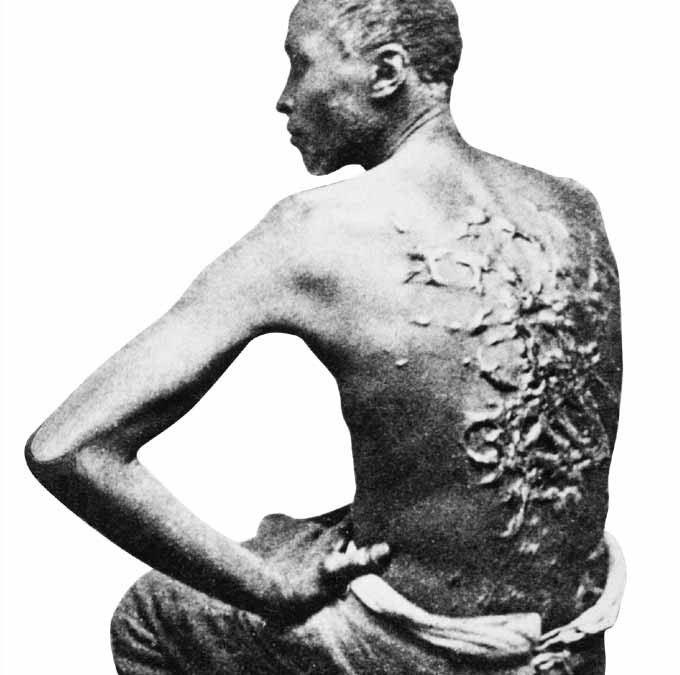
All of this “hidden” information about his experiments was told by author John Brown who was part of the experiments as a slave but managed to escape in the 1830s and migrate to England where in 1855 he published an autobiography titled Slave Life in Georgia in which he describes with detail the atrocious experiments he had to face. As anesthesia was still not invented (it would be invented in 1846), all the experiments were done on live flesh with knives, saws, and scalpels.
John Brown also describes the dementia Hamilton suffered, as he kept saying that “you are more resilient to pain than we are” but all he could hear was screams of excruciating pain. The “treatment” that John Brown received from Hamilton was blisters on his arms and legs every two weeks in order to prove that Brown’s skin was thicker. This went on for nine long months to the point where the experiment wasn’t able to prove the myth.
Even if Hamilton’s experiments were not justifying his theory, he kept telling people that Black people feel less pain, with others spreading the myth and exaggerating by saying that “Black people feel no pain”. Sadly, Hamilton wasn’t the only doctor to do experiments on Black people. Many other doctors around America and even Europe believed this myth to the point where they would actually apply it to their patients.
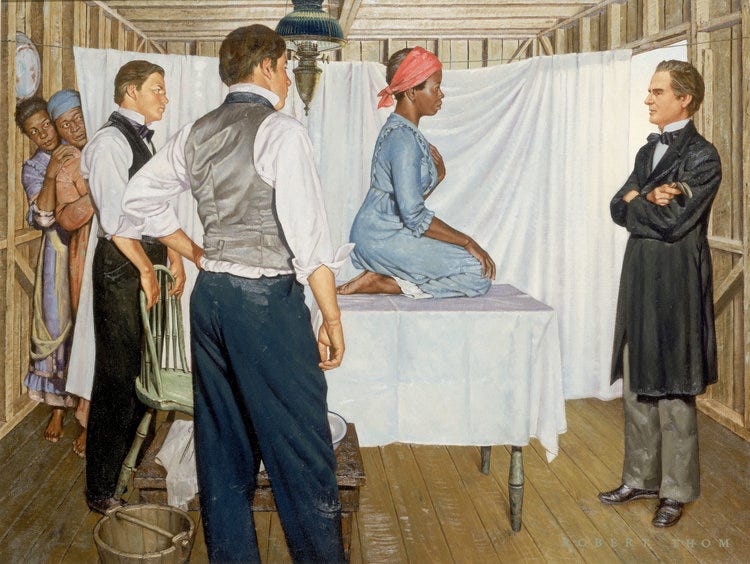
Dr. J. Marion Sims, also known as the “father of gynecology” was one of the doctors who actually believed in this myth. Many of his risky surgeries were usually performed on Black people as he believed they had a better chance of survival. As a specialist in gynecology, he made many discoveries in the field by performing experiments on enslaved Black women.
Many of his surgeries included vesicovaginal and rectovaginal fistulae which back in the day was quite a complex procedure due to the lack of technological advancements. To give you a short description for a better understanding, a surgery that opens into the urinary tract is called a vesicovaginal fistula and the surgery to cut into the rectum is called a rectovaginal fistula.
Most of his experiments took place from the 1850s until slavery was abolished. What is important about this date is the fact that by 1850, anesthesia had been invented, therefore Sims was only giving anesthesia to his white patients as he believed that “Black people don’t feel pain, therefore why waste the anesthesia?”
Both Sims and Hamilton have been seen as very valued doctors within their specific fields as well as trustees of the Medical Academy. That is the reason why so many people believed their myth and integrated it into the medical society as a “fact”.
Using the myth to justify slavery
In their ideology and theories — which were supported by many other scholars within the field — they tried to actually justify the reason why Black people had been enslaved by using their so believed “higher resilience to pain”. They even went further by saying that Black people were always meant to be slaves because of their high physical performance as well as high physical endurance (resilience to pain). In all of their writings, they tried to assess Black people by always comparing them to white people, but very rarely to other races.
In 1787, British Dr. Benjamin Moseley wrote a manual named A Treatise on Tropical Diseases where he defined that slavery of Black people is justified by their weak lungs which can only be strengthened through hard work (in the manual described as intensive labor). He also goes on, trying to support an early ideology of the resilience of Black people to pain by saying that “Black people can bear surgical operations much more than white people.” He goes on to describe his experience of amputating the limbs of Black people which he allegedly says “would have held the upper part of the limb themselves during surgery.”
What is even more surprising is that Thomas Jefferson was actually supporting all of these ideologies in his Notes of the State of Virginia by stating that the difference between Black and white people is “the real distinctions which nature has made.” This is where we can see a pattern creating from mythological ideologies and theories that are supported by contemporary society because they were presented by powerful people. To give a better understanding, in the 19th and previous centuries, if you were rich, you were “intelligent”, therefore respected.
I am not trying to say that the scholars mentioned above were not intelligent but making up theories which you can’t even prove through years of experimentation does not really show much intelligence. It was this circle of powerful white people in 19th century America that controlled the society and their beliefs.
To make it more clear, their main argument was that due to the Black people’s natural “distinctive differences” they should be in a certain place within society, and the white privileged, powerful men should be at the top as they somehow are all born as leaders of the world.
There are lots of other examples from other such powerful people that are trying to define this ideology through the 19th century, but I presume that you all get the gist at this point. They are not only guilty of constructing a myth that has only provoked unnecessary suffering through the excruciating pain of thousands of Black people, but also because they actually tried to justify slavery to society.
Don’t think that society is much different now, maybe people are more educated, yes, but they are still as naive as in the early centuries, maybe even more than before. Therefore our present society is much more vulnerable to this sort of created mythology that can be easily believed and supported like a religion due to social media.
40% of medical students are still taught this myth
As we historians say, what is in the past is in the past and sadly we cannot change it, but at least we can analyze it to get a better understanding. From the numerous historical resources that are present on this issue, it is sublime how so many medical students still endorse this myth even if it has been proven over and over again by scholars from the medical field that the myth is only a lie.
A good piece of evidence that disproves this myth is found in Professor Lundy Braun’s book Breathing Race into the Machine: The Surprising Career of the Spirometer from Plantation to Genetics published in 2014. Professor Braun from the Brown University Department of Medical Science and African Studies has been working for years to disprove this myth. Yet this myth described by Professor Braun as “race correction” is still being lectured to medical students and even present in textbooks.
In a study from 2016 published by the Proceedings of the National Academies of Science of the United States of America, it has been discovered that 40% of first and second-year medical students supported the belief that “Black people’s skin is thicker than white people’s.” This is because many scholars from the medical field — especially in America — still believe this myth, despite years of pointless research in trying to prove something that that does not exist.
Especially, with the effect it causes on students when seeing the same myth being published in core textbooks over and over again, year after year, even you as a junior student in the medical world could easily fall in believing this myth. It is not only the students that are to blame, but the very aristocratic and authoritarian teachers found within medical schools. Of course, they have to be severe because this is something very serious that will lead to them saving lives.
However, at the same time, they don’t allow students to have their own word as these medical scholars sometimes forget that they are human, therefore they can make mistakes. In Business School, I sometimes corrected my lecturers and they appreciated it as well as excused themselves by saying that they are human, not textbook robots.
Talking about textbooks, there has been a huge incident which provoked a lot of scandals with a London based publisher by the name of Pearson who had published in a medical core textbook a section that describes the response to pain based on cultural differences. This is not only racist to Black people but all other ethnic groups around the world. The book is called Nursing: A Concept-Based Approach to Learning by Pearson Education Publishing.
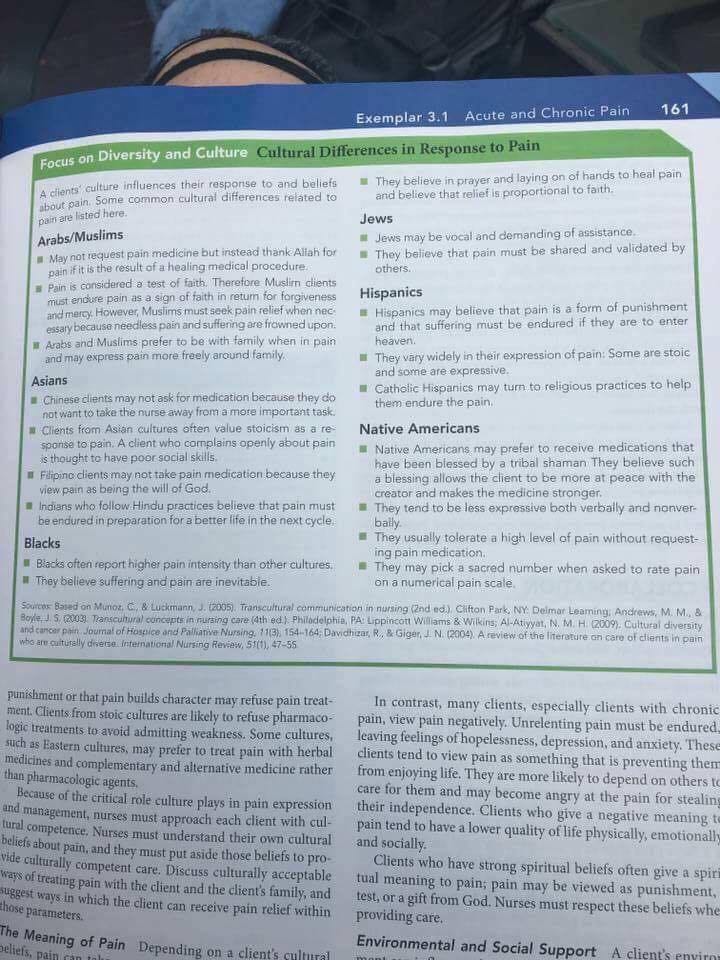
This started a major scandal in 2017 where Pearson actually pulled back all the 2017 textbooks to remove the section on “Cultural Differences in Response to Pain.” The scandal was started by a medical student that had posted this specific page of the textbook on Facebook and described it as the most racist thing the student had ever seen.
The publication responded with a few tweets saying that they would remove the offensive section from the book and assure that future copies would be curated before publishing.
However, by this point, I feel that this ideology has been heavily indoctrinated so much that it has become a common practice or “basic knowledge to know” within the medical field. The material taught to medical students goes as far as emphasizing that this “hidden bias” is not intentional, but an actual fact that “many patients are not aware of.”
The myth applied in hospitals today
Besides seeing this still being taught in medical schools, we see this in practice across many hospitals within America as well as other parts of the world. In another research paper published by Proceedings of the National Academies of Science of the United States of America, it has been assessed that this “hidden bias” is happening within hospitals. Many residents and even senior medics are undertreating Black patients as if they were more resilient to pain.
A second study was performed by the same research team just to find out that on average, half of the medics within a United States hospital still endorsed the belief in this myth. Other findings are even more worrisome, with a study from 2012 that had discovered many pediatricians unconsciously proceeding with racial bias in treating the pain of Black patients with prescriptions that included less to no painkillers compared to the prescriptions to white patients.
The analyses of research papers based on racial bias in treating pain by medical scholars over the past 20 years have led to some surprising results such as a Black person being 22% more likely to not receive any pain medication with their prescription.
These studies all prove that this myth still fuels inadequate treatment that is based on racial prejudice described as hidden bias by scholars in this specific field.
What is extremely imperative for everyone reading this article to understand is that every person, no matter their skin color or background, processes pain in different ways and has different levels of pain endurance.
I had small surgeries performed on me at a younger age where I wasn’t given any anesthetic because this would have risen the chances of complications, and this is why I believe I have slowly build up my pain resilience. The point that I am trying to make with this statement is that we aren’t necessarily born with a specific pain endurance level, but this is more developed during life based on different medical experiences.
A more recent study from 2019 shows how this racial bias keeps evolving to new levels. A group of medics has been asked to identify the pain expressed by patients in different photos. The participants recognized pain much easier from the faces of white patients compared to the faces of Black patients. The participants were shown the results and they said that these racial disparities in assessing the pain level of Black patients were not intentional. Scholars once again show that any medic is as likely to commit unconscious bias. (Here is a link to the research paper mentioned above.)
From this, they have analyzed that it is not necessarily medics being racially prejudiced against Black people, but that they have been so indoctrinated with this myth that they truly believe it as if it was written as part of the holy scripture. This is why if we are not able to open the eyes of certain medical scholars that still believe and teach this myth, we need to open the eyes of students who might be able to abolish this myth in the near future.
Medics need to stop underestimating the pain of Black patients because the underprescribing medication can lead to future medical complications or medical problems that haven’t been treated at the right time with the right medications, getting worst to the point where surgery may be needed. Thank God there are regulations set in place by WHO (World Health Organisation) which state that anesthesia must always be used with the exception of anesthesia creating possible complications or raising the failure risks of surgery.
To be more critical on the severity of the problem, I have found a study conducted in 1997 examining pain management among patients with metastatic cancer found that only 35% of racial minority patients received the appropriate prescriptions. We are talking about cancer patients, giving the wrong prescription to such vulnerable patients can have lethal consequences. So, I don’t think I need to further emphasize how serious this issue is and how urgently we need to abolish this myth.
How can we abolish this myth?
This problem has also been created by the lack of data collection that is happening in major hospitals. Medics should collect every piece of data from a patient, this also includes the pain management of the patient based on how many painkillers he has been prescribed based on other personal information such as the ethnicity of the patient. With this sort of data, we can not only prove that racial bias exists in certain hospitals, but we can also assure that racial biases are being abolished in other hospitals.
Another good way to abolish this myth from hospitals is to standardize the process of pain analysis by having each medic follow specific guidelines when coming up with a diagnosis and offering a prescription. By implementing a systematic approach to the process of diagnosis and medical prescription, we can remove individual discretion which translates to removing this hidden bias undertreating people of other races. The AAPM (American Academy of Pain Medicine) is working towards implementing specific guidelines for medics to follow when treating different types of pains patients might present.
Researchers are looking at more technologically advanced ways of analyzing pain, not only because of this hidden bias but also because patients don’t always know how to describe the type of pain they are feeling, as well as seldom medics don’t correctly estimate the type of pain felt by the patient. Therefore researchers are developing a blood test that uses biomarkers that can analyze the type of pain felt by the patient as well as its intensity.
However, besides all these implementations within the medical system, we need to make people aware of this myth. The more people know the truth behind this myth the higher the chances of this truth being spread around the world in order to stop this hidden bias and racist action despite it being with or without intention.
Avid Writer with invaluable knowledge of Humanity!
Upcoming historian with over 30 million views online.
“You make your own life.”
